
A nervous patient (in his mid-20s) presented at the practice unhappy with his smile and the shade/shape of his anterior teeth, which was affecting his self-confidence. He reported no acute pain. He wanted to have his teeth treated, but was unprepared to have fixed braces at his age. He sought to have braces that were invisible and did not regress his confidence further.
His last dental visit was more than four years ago due to a traumatic past experience. He was referred to the practice through a friend.
As with any assessment, we started off discussing the patient’s main concerns and build a rapport with him so he felt at ease. We then moved on to discussing his medical history and social history.
The patient was generally fit and well, taking no medication and no known allergies. Alcohol consumption was moderate and he was a non-smoker. Furthermore, his oral hygiene was good, brushing twice daily with an electric toothbrush and occasional flossing.
<Slider>
Extraorally, no signs of any pathology and all were functioning within the normal parameters. Intraorally, all the soft tissues were within the normal limits and no signs of pathology were visible apart from generalised marginal gingivitis. He had a thick bio-type.
Regarding dentition, there was an enamel fracture on the UL1, missing teeth and multiple restoration present.
Orthodontic review:
An OPT was taken to assess for any pathology in the upper and lower arch. Caries identified on LL8MO and peri-apical pathology under LR5.
When tested, the LR5 was not tender to percussion and gave a negative response to ethyl chloride.
The results of the extraoral and intraoral examinations are summarised in a problem list (Table 1). Based on this list, an interdisciplinary approach helped to define all the potential treatment goals.
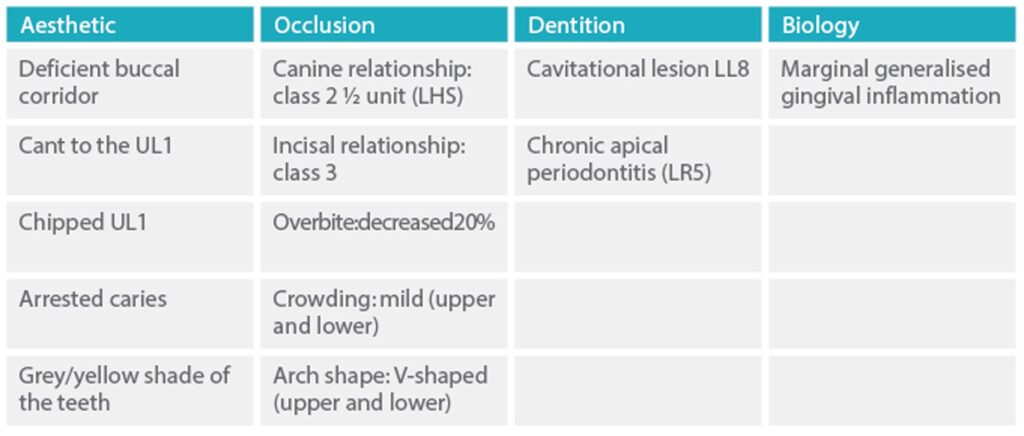
Table 1: Problem list
The scope of the treatment goals achievable were presented to the patient with advantages and disadvantages of the alternative treatment plans. The treatment goals (listed in Table 2) were agreed and defined.
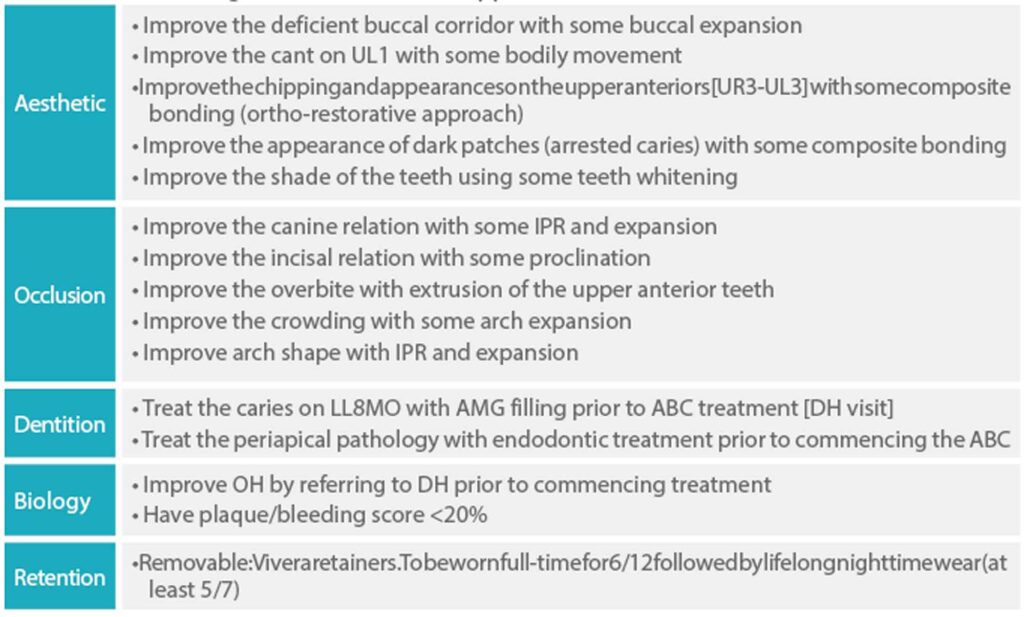
Table 2: Treatment goal (non-extraction approach)
Clincheck treatment planning
Specific instructions were provided in the form of a four-sentence prescription to the Invisalign technician and included the following:
Patient’s chief complaint: patient does not like his smile at all. Please improve the upper and lower crowding and widen the smile. Level the gingival margins of the upper anterior teeth. No movements on the LR5 until aligner number 12
Anterior reference point: tip UR1 1mm buccally and use this to align the upper anterior teeth
Posterior reference point: use the distobuccal cusp of the upper sevens to widen the smile
Overjet/overbite: please provide an overjet of 3mm and overbite of 30%.
Treatment summary
The original treatment plan included 15 aligners on the top and bottom arch. Optimised attachments were placed on the upper arch from UR5 to UL5 and on LL6 to LL4 and LR3 to LR6 (Figures 11-13).
<slider>
The patient completed his alignment journey with 15 aligners on top and lower. No refinements/additional aligners were needed. This equated to a treatment time of approximately four months.
This was based on the patient being fully compliant and wearing each aligner for seven days with at least 20 hours’ wear a day. The patient was asked to replace the aligners at night to ensure it inflicted minimal pain.
B: Bleaching
To lift the shade of the teeth, Boutique Hybrid Pro whitening (syringes) was carried out while the patient had his aligners on from day one.
The patient was asked to continue doing the whitening until he was happy with the shade (continued whitening up to week 10 going through 2.5 syringes).
To get the best possible outcome, the patient was recommended and shown to apply a pea-size amount of gel on his aligners every night.
The peroxide diffuses through the composite buttons and lifts the shade of the dentine; effectively saving time for both the clinician and the patient. Figures 14 to 22 show the post-treatment photos. The patient’s initial main concerns of his smile alignment, shade and crowding were all resolved. An improved inter-incisal angle and contact were created.
<slider>
C: Contouring
An acceptable aesthetic result was achieved with minimal restorative work. Additive bonding was applied to the upper anteriors to improve the shape and shade of the teeth.
Furthermore, the arrested caries on the buccal surface of UL4 was treated with Icon and composite bonding.
The composite bonding was done under strict regime of rubber dam isolation to ensure a safe environment and appropriate moisture control.
The non-working/adjacent teeth were isolated with polytetrafluoroethylene (PTFE) tape. The composite chosen for this case was Ivoclar Empress BL-XL shade, as it exhibits high physical strength under compression.
The composite was heated using the C-Flo from Bryant Dental at 44oc to allow a smooth flow. Optrasculpt from Ivoclar was used to apply and blend the composite to the existing tooth surface.
The polishing was done using Optragate and polishing spirals and points to achieve a high lustre, respecting the tooth anatomy.
Figures 23 to 26 demonstrate the improvement of the smile using a combination of orthodontic, whitening and additive composite bonding.
Following the contouring process, the patient was ecstatic to see his final smile revealed.
Although the patient had seen the trial smile at an earlier stage in the treatment, he had not fully appreciated what could be achieved with composite or the difference it would make.
The patient was really happy with the outcome, so we decided that the treatment should be concluded.
An intraoral scan was done using the Itero to fabricate the Vivera upper and lower retainers for lifelong night-time wear.
The retainers are 0.4mm thick and can also be used for any future tooth whitening.
<slider>
Invisalign can be used for a variety of cases from simple to complex; however, it is the responsibility of the dental clinician to work within their comfort zone as well as their capabilities.
For me, the biggest advantage of using Invisalign is the ability of having a Clincheck to demonstrate to the patient exactly what results can be expected at the end of the aligner journey.
These days, with the use of digital smile design, we can go one step further and use the STL file to do a digital mock-up on the final teeth position, showing the outcome of any contouring work (prosthetics and/or composite).
Products used:


Showing our patients how to get the most out of their tooth cleaning routine is one of the most important services we…
READ MORE
If you’re brushing your teeth twice a day consistently, and yet you keep developing decay, you might feel like you’re fighting a…
READ MORE
Tooth grinding is becoming an increasing problem, in huge part due to the increased levels of daily stress in the busy (and…
READ MORE
Valentine’s Day is the perfect time to give your smile some love. But not always to impress someone else though - most…
READ MORE
We understand how discerning patients are when they are looking for dental treatment. In 2025, meeting patients’ needs means harnessing the latest…
READ MORE
Many private dental practices reduce their offering during the Christmas break, and it can be challenging to access an emergency appointment. But…
READ MORE
Christmas is one of the most stressful times to be hit with a dental emergency, mainly because it can be incredibly hard…
READ MORE
There is now a close link between gum disease and diabetes, based on countless conclusive clinical studies. As dentists, we feel a…
READ MORE
The toothbrush you choose can have an impact on your oral hygiene, and the condition of your teeth. Whilst electric toothbrushes have…
READ MORE
One of the questions we are asked most by patients is “Does it matter which mouthwash I use?” A great question, especially…
READ MORE
Periodontal treatment is one of our stand-out areas of expertise here at Meliora Dental. Part of this service includes treating excess gum…
READ MORE")
What an incredible 18 months it’s been since we established Meliora Dental! We’ve recently been reflecting on our journey so far since…
READ MORE
Believe it or not, we’ve actually had patients tell us they love their new dental implant smile more than they loved their…
READ MORE
Gum disease is the silent assassin responsible for the millions of missing teeth across the UK. It can be hard to spot,…
READ MORE
Gum health affects your wider health more than you might think. With compromised gum health, you risk doing damage to your cardiovascular…
READ MORE
A missing tooth can cause more problems than simply a gap in your smile. In fact, leaving tooth replacement too long can…
READ MORE")
Gum disease remains the main culprit for premature tooth loss in adult patients here in the UK. If you’re searching ‘gum disease…
READ MORE
There is a bigger spotlight than ever on the impact the food and drink we consume can have on our health, and…
READ MORE
The human heart works in mysterious ways. But, thanks to a surge in clinical research over the last couple of decades, we…
READ MORE
Kunal Rai recently shared his insights on the transformative impact of artificial intelligence in the field of dentistry with Dentistry.co.uk, the leading publication…
READ MORE")
As with many other emergencies in life, dental emergencies can strike when you least expect them. Here at Meliora Dental, we more…
READ MORE")
Summertime is on its way in… finally! With summertime comes the season for many outdoor events, including weddings. 40% of weddings take…
READ MORE")
One of the greatest dental myths still doing the rounds in 2024, is that there comes a time when age becomes a…
READ MORE")
Let’s begin by answering this question. Yes. Certain gaps in your teeth can be closed without the use of braces. The technique…
READ MORE")
What if there was a way of doing small things to your teeth that would have a big impact on the appearance…
READ MORE")
For many people, tooth replacement is likely to be up there with some of the biggest undertakings they’ll ever make in their…
READ MORE")
Invisalign is the leading clear aligner technology brand. Since 2000, this removable teeth-straightening protocol has helped over 17 million people achieve a…
READ MORE
If you’re a regular reader of the news, you’re likely to be aware of the problems people across the UK (perhaps yourself…
READ MORE
We are proud to announce the launch of our much awaited new website. We hope you enjoy using it and find the…
READ MORE
Kunal Rai discusses the use of social media in the dental profession, including both advantages and disadvantages, and how to use it…
READ MORE
Kunal Rai explains how AI has enhanced his practice, from streamlining processes to improving the reliability of diagnoses. Please tell us a…
READ MORE
Kunal Rai discusses his most rewarding experience in dentistry, his ambitions for the future and what he’s passionate about away from work.…
READ MORE
Kunal Rai presents a multidisciplinary case highlighting how careful case selection, assessment and treatment planning can provide an excellent outcome for patients…
READ MORE
Kunal Rai presents a case report of a smile makeover using an align, bleach and contour approach. A patient in her mid-twenties…
READ MOREBoost the way you look and feel with our facial aesthetic treatment options.
EXPLORE

Dental Phobia Certified

Winner : AGC Case of the Year 2022

Orthodontics : Clear Aligner

Best Young Dentist 2021 Finalist

Best Young Dentist 2020 Finalist
As a result of an accident I had as a child my front tooth suffered some trauma and became discoloured over time. The tooth eventually broke last year which led to it being removed. I was referred to Kunal who took me through the various options I had. As functionality was the most important aspect...
As a child, I was given a fixed brace by a practice who showed very little care. These were removed after 9 months due to them being "unable to straighten anymore" leaving me unhappy with my teeth and a major open bite. As years went on, I became less and less confident with my teeth,...
Thank you for your hard work and I hope this testimonial reflects just how happy I am with my smile. The care and attention which I received during my smile makeover was far better than any I have previously experienced. Kunal and his team were amazing throughout the entire process. I had regular check-ups throughout,...
Kunal is a very approachable, informative and meticulous dentist. From the beginning of my last Invisalign journey, Kunal explained the procedure very clearly and thoroughly. He showed me a 3D image and how my teeth would change throughout the treatment, the length of the treatment and the possible cons of it, such as black triangles...
I was never conscious of my teeth much but over the years my teeth became more overcrowded, in particular my bottom teeth. I found myself smiling in photos with my mouth closed as I didn’t like the way my teeth looked this was something that over time I got even more conscious of and so...
Kunal and his team gave me the best experience throughout my transformation. Everything was explained all the way through the process and he even accommodated my lunch time appointments every 4 weeks! He always gave his honest opinions and made me feel at ease. He is such a perfectionist and wouldn’t let me leave my...
As a result of an accident I had as a child my front tooth suffered some trauma and became discoloured over time. The tooth eventually broke last year which led to it being removed. I was referred to Kunal who took me through the various options I had. As functionality was the most important aspect for a replacement for me we agreed an implant was the route to go. The tooth removal however left an element of damage to the natural bone so I had to undergo a bone graft to repair this. One year after the extraction (as 2 bone grafts were needed in the end) I'm now fitted with my implant and I can honestly say I have never been as proud to smile as I am today. From start to finish Kunal...
As a child, I was given a fixed brace by a practice who showed very little care. These were removed after 9 months due to them being "unable to straighten anymore" leaving me unhappy with my teeth and a major open bite. As years went on, I became less and less confident with my teeth, until I came across Kunal. From the first moment I walked into the practice, Kunal was very welcoming and talked me through every possible stage that would happen if I was to go ahead with treatment with zoom calls to show the perceived results and ensure I was happy to go ahead with treatment Kunal gave me a diagnosis of my open bite, which was behavioural, therefore instantly this behavioural trait was worked upon to receive the best results from...
Thank you for your hard work and I hope this testimonial reflects just how happy I am with my smile. The care and attention which I received during my smile makeover was far better than any I have previously experienced. Kunal and his team were amazing throughout the entire process. I had regular check-ups throughout, and each time Kunal would make sure I was happy, not just with the work that had already taken place, but with the direction my smile was headed. Kunal engaged in discussion with me about each aspect making sure I fully understood what would happen and giving me the chance to have my own input. This combined with his vast knowledge and incredible skill left me feeling fully relaxed and in safe hands. Each step was performed in meticulous detail,...
Kunal is a very approachable, informative and meticulous dentist. From the beginning of my last Invisalign journey, Kunal explained the procedure very clearly and thoroughly. He showed me a 3D image and how my teeth would change throughout the treatment, the length of the treatment and the possible cons of it, such as black triangles and what can be done to minimize them. Kunal made it clear from the beginning that as a dentist his interest was the function of the teeth, better oral hygiene, the bite etc. I learned so much from him regarding my own teeth, that it was my bottom teeth that was causing the misalignment on my top teeth, l have gum recession due to excess brushing and l was in danger of losing two teeth due to it! Things my...




















![Nadia Ahmed [Leeds]](https://lh3.googleusercontent.com/a/ACg8ocIz84NAs6PBSMcyee1Gg49Hhu25xQ31m0qBfHV55QolomX2wQ=s128-c0x00000000-cc-rp-mo)


















































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}